...that is to say, why does obesity exist & how does it work?
The physiologic causes of obesity (etiology) are somewhat straightforward, but why obesity exists in such large scale is not yet understood. At its most basic level, obesity is an energy imbalance - the body is not burning as much potential energy (metabolism & exercise) as it consumes (food), and so that energy is stored (as fat). When this imbalance persists for a long time, fat stores eventually become much larger than the body needs.
There are two types of obesity - primary and secondary. Primary obesity is the most common form - it occurs when someone consumes many more calories than their body uses. Think of it as too much energy available. Secondary obesity occurs because the body doesn't use enough energy in its daily functioning. This isn't necessarily related to someone just not exercising, though of course that would make the problem worse. Secondary obesity can be caused by abnormal metabolism function (as in hypothyroidism), defects in a chromosome, or a problem with the central nervous system (Lewis, 2014).
Because primary obesity represent the majority of cases, that is what I will focus on. There are many factors to consider as to why people become obese.
One component is genetic - based on their inherited genes, some people are much more likely to become obese.
Genetics impact how our body stores and uses energy. In more ancient times, genes that promoted energy storage were favorable - this increased the chances of surviving famines. In modern American culture, the great abundance and cultural significance of food makes a genetic predisposition to storing energy unfavorable. "Estimates of obesity as an inherited problem are more than 50%" (Lewis, 2014). However, unless these genes cause a form of secondary obesity, it is likely that genetics alone only increase susceptibility to obesity - behavior (diet and exercise habits) still play a significant role (CDC, 2012).
The environment also has an impact on obesity's development. Food, especially processed foods, is easily accessible and very visible in the Western world.
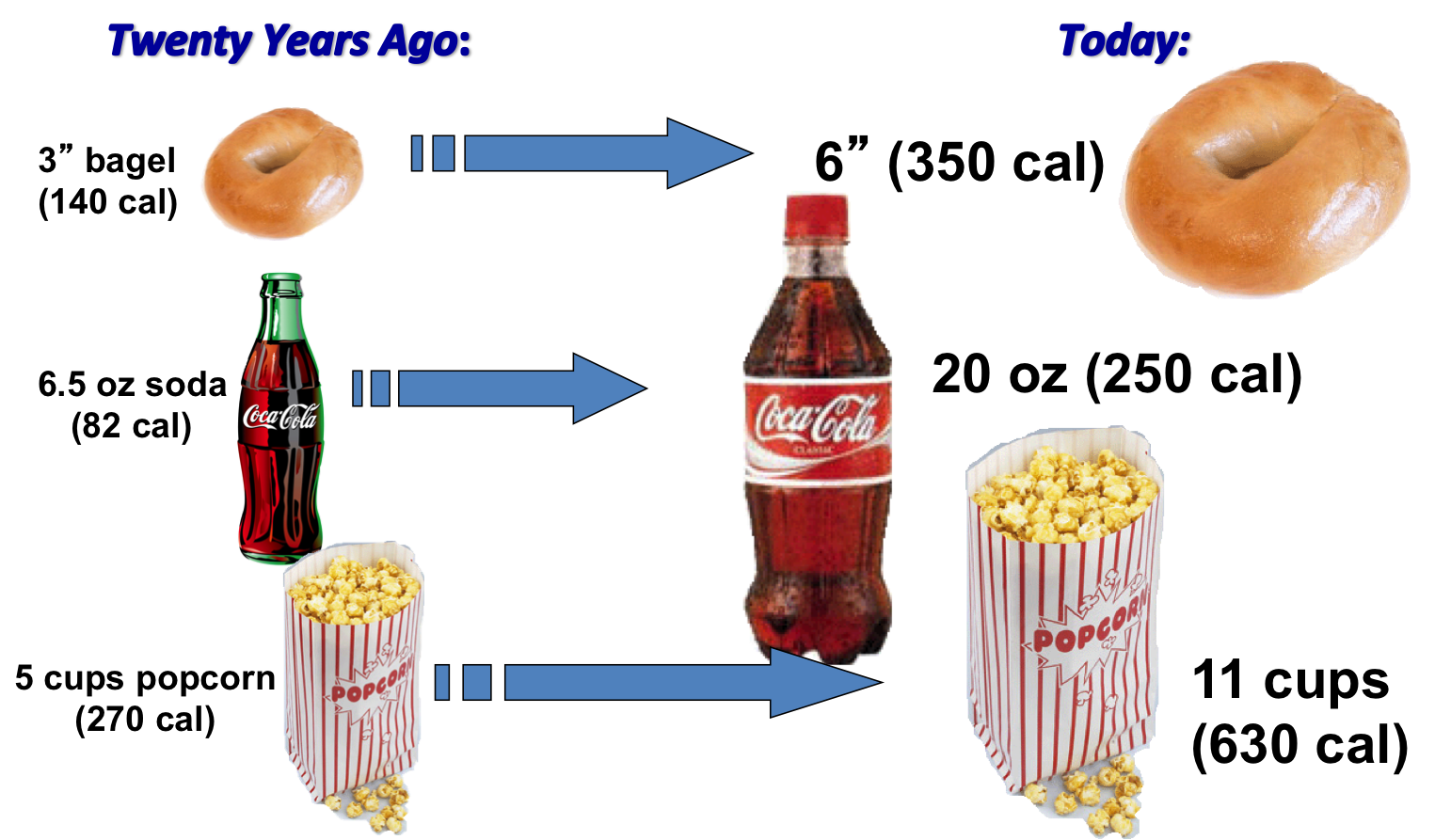
Portion sizes have increased, and empty calories are readily available at every gas station and food mart. Often these processed foods are cheaper to buy in bulk than fresh foods, and so people with lower income may resort to eating less nutritious foods to save money. Neighborhoods may be unsafe for outdoor activity, and transportation to grocery markets that sell fresh foods may not be reliable. Many jobs are sedentary, and much free time is spent watching TV or on social media.
There are cultural and social elements that promote overconsumption of foods. Food is symbolic - the average American cannot look at a Thanksgiving spread and think only of nutritional value. It is associated with family, reward, celebration, comfort, home.
These pleasurable associations with food can result in overeating in times of stress or discomfort. "When overeating develops at an early age and continues into adulthood, one's ability to sense fullness (satiety) is compromised. Whether triggered by specific food or by the wide variety of choices, some people consume more food than their bodies need. The lack of hunger that drives eating has been termed "mindless eating" and leads to consumption of unnecessary calories and increase in body weight" (Lewis, 2014, pp. 910).
Finally, there are hormones and signaling proteins called peptides which play a role in appetite. Ghrelin is made by the stomach after it has been empty for a while, prompting hunger. Ghrelin levels decline when food is in the stomach. In obesity, ghrelin levels do not decline with food intake, and so the body doesn't have the sensation of fullness when it normally would. Leptin is made by fat cells, and suppresses hunger. In obesity, leptin levels are actually increased, meaning that obese people likely have a resistance to leptin and can no longer feel its effects (Lewis, 2014, pp. 909)
As fat cells increase in size and number to the point of obesity, the body faces many increased health risks. These include heart disease, sleep apnea, asthma, high blood pressure, type 2 diabetes, chronic kidney disease, and many other health problems. I will discuss these in greater length in a future blog post.
Lewis, S. L. (2014). Obesity. In Harding M. M. (Eds.), Medical-Surgical Nursing - Assess and Management of Clinical Problems. (pp. 906 - 922). St. Louis, Elsevier.
Centers for Disease Control and Prevention. (2014). Overweight and Obesity - Data and Statistics. [Graphic Illustrations]. Retrived from http://www.cdc.gov/obesity/data/prevalence-maps.html













{kind=link}
{kind=link}
{kind=link}
{kind=link}